Traumatic head injuries in cats
Written by Simon Platt
The ability to recognize clinical signs consistent with a declining neurologic status is critical in the management of cats following head trauma. Trauma significant enough to cause brain injury will have systemic effects, which may be life-threatening.
Warning
This article contains sensitive photo that may be harmful for young children

Key points
A thorough systemic evaluation of any cat which has been involved in a traumatic event is essential prior to focusing on the nervous system.
The neurologic exam of the head-injured cat can be condensed into assessment of mentation, limb function and pupillary light reflexes.
Imaging the brain of the head trauma cat can help identify causes of the neurologic dysfunction, but rarely leads to a surgical treatment.
Fluid therapy is essential for all cats which have suffered a head injury and should focus on restoring systemic blood pressure.
Flow-by oxygen therapy is recommended as a first-line treatment for cats with traumatic brain injury.
Introduction
The ability to recognize clinical signs consistent with a declining neurologic status is critical in the management of cats following head trauma [1] [2] [3] [4]. Trauma significant enough to cause brain injury will have systemic effects, which may be life-threatening. Additionally, systemic injuries and shock will cause continued decline in the head trauma patient, and a complete systemic evaluation and stabilization is therefore required in addition to a thorough neurologic assessment, as summarized in Table 1.
| Parameter | Suggested goal | Suggested treatment |
|---|---|---|
| Neurologic examination | Modified Glasgow Coma Scale (MGCS) > 15 |
Ensure head elevation (30º)
Ensure all points below are addressed
Consider mannitol (see below)
Consider surgery (see text)
|
| Blood pressure | MAP 80-120 mmHg |
Adjust fluid therapy
Pressor support (dopamine 2-10 µg/kg/min)
|
| Blood gases |
PaO2 ≥ 90 mmHg
PaCO2 < 35-40 mmHg
|
Oxygen supplementation
Consider active ventilation
|
| Pulse oximetry | SPO2 ≥ 95% |
Oxygen supplementation
Consider active ventilation
|
| Heart rate & rhythm |
Avoid tachy- and bradycardias
Avoid arrhythmias
|
Adjust fluid therapy
Treat for pain
Address ICP
Treat arrhythmias specifically
|
| Central venous pressure | 5-12 cm H2O | Adjust fluid therapy |
| Respiratory rate & rhythm | 10-25/min | Ventilate if necessary |
| Body temperature | 37-38.5 °C (98.6-101.3 °F) | Passive warming or cooling |
| Electrolytes | See individual laboratory normal values | Adjust fluid therapy |
| Blood glucose | 4-6 mmol/L (67-168 mg/dL) |
Adjust fluid therapy
Consider dextrose administration
|
| Intracranial pressure | 5-12 mmHg | As for MGCS abnormalities (see action plan in Figure 4) |
Systemic assessment
Initial assessment should involve evaluation of the patient’s respiratory and cardiovascular system. A patent airway must be established and maintained, if necessary via endotracheal intubation. Breathing patterns may be affected by thoracic trauma but can also be secondary to brain injury. Auscultation of the thorax may detect pulmonary pathology or cardiac arrhythmias. The cardiovascular system should be evaluated by monitoring heart rate, blood pressure, and electrocardiography. An electrocardiogram may demonstrate cardiac arrhythmias secondary to traumatic myocarditis, systemic shock, or brain injury. Arterial blood analysis and lactate concentrations may provide additional information regarding systemic perfusion and respiratory function [1] [2] [3] [4].
Once the patient is stable, radiographs of the chest and abdomen are recommended to evaluate for pulmonary contusions, pneumothorax, and abdominal injuries. Pulmonary contusions are common following trauma and may not be at their most severe until 24 hours after injury. Trauma can also result in injury to abdominal organs; the abdomen should be evaluated via radiography and ultrasonography for the presence of free fluid, such as blood or urine, which may require additional therapy. Radiographs of the cervical vertebrae should also be considered, as head trauma can often be accompanied by fractures and luxations of these bones.
Neurologic assessment
Neurologic assessment should be undertaken on all head trauma patients [1] [2] [3] [4] [5]. Assessment of neurologic status should initially be performed every 30-60 minutes; frequent assessment allows for monitoring efficacy of treatment and early recognition of a deteriorating status.
A scoring system, the Modified Glasgow Coma Scale (MGCS), has been developed in veterinary patients to provide an objective assessment and allow for rational diagnostic and treatment decisions. The scale evaluates three categories — motor activity, brainstem reflexes, and level of consciousness — enabling initial and serial monitoring in patients following injury (Table 2). Each category is evaluated using objective standards and scored between 1 and 6, with lower scores assigned to more severe clinical signs. The score from each category is added together to determine a patient’s coma score, ranging from 3 to 18, and may be used to guide treatment decisions and prognosis [5].
| Motor activity | Score | Brainstem reflexes | Score | Level of consciousness | Score |
|---|---|---|---|---|---|
| Normal gait, normal spinal reflexes | 6 | Normal pupillary light reflexes and oculocephalic reflexes | 6 | Occasional periods of alertness and responsive to environment | 6 |
| Hemiparesis, tetraparesis or decerebrate activity | 5 | Slow pupillary light reflexes and normal to reduced oculocephalic reflexes | 5 | Depression or delirium, capable of responding but response may be inappropriate | 5 |
| Recumbent, intermittent extensor rigidity | 4 | Bilateral unresponsive miosis with normal to reduced oculocephalic reflexes | 4 | Semicomatose, responsive to visual stimuli | 4 |
| Recumbent, constant extensor rigidity | 3 | Pinpoint pupils with reduced to absent oculocephalic reflexes | 3 | Semicomatose, responsive to auditory stimuli | 3 |
| Recumbent, constant extensor rigidity with opisthotonos | 2 | Unilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes | 2 | Semicomatose, responsive only to repeated noxious stimuli | 2 |
| Recumbent, hypotonia of muscles, depressed or absent spinal reflexes | 1 | Bilateral, unresponsive mydriasis with reduced to absent oculocephalic reflexes | 1 | Comatose, unresponsive to repeated noxious stimuli | 1 |
Assessment of limb function
The first category describes a patient’s motor activity, limb tone, and posture. Voluntary motor activity is characterized as normal, paretic, or recumbent. Patients typically maintain some degree of voluntary motor activity, even in altered states of consciousness, unless comatose. Abnormal motor function usually reflects either brainstem injury or spinal cord injury; the latter may complicate the assessment of head trauma [5].
An animal’s posture after head trauma can also provide information about the location and degree of brain injury. Decerebrate rigidity (Figure 1) can occur following cerebral trauma and suggests severe brain injury; this posture carries a poor prognosis, as it reflects loss of communication between the cerebrum and the brain stem. Animals with decerebrate rigidity have opisthotonos with hyperextension of all four limbs and are stuporous or comatose, with abnormal pupillary light reactions. This should be differentiated from decerebellate rigidity, which suggests acute cerebellar damage and may cause either flexion or extension of the pelvic limbs; however, consciousness may be normal.

Assessment of brainstem reflexes
Pupil size, the pupillary light reflex, and the oculocephalic reflex should be immediately evaluated in all head trauma patients. Pupil size, symmetry, and reactivity can provide valuable information about severity of brain injury and prognosis, and these parameters should be frequently re-assessed as they can signal a deteriorating neurologic status. Response of the pupils to a bright light indicates sufficient function of the retina, optic nerves, optic chiasm, and rostral brainstem. Bilateral mydriasis that is unresponsive to light can indicate permanent midbrain damage or brain herniation and suggests a poor prognosis (Figure 2). Progression from miosis to mydriasis indicates a deteriorating neurologic status and is an indication for immediate, aggressive therapy. Unilateral changes in pupil size may be seen early in deterioration. Paralysis of cranial nerve (CN) III can lead to mydriasis, loss of direct pupillary light reflex, ptosis, and ventrolateral strabismus. The CN III nucleus is located in the midbrain; therefore, damage to this nucleus can be indicative of midbrain injury or compression secondary to transtentorial herniation [5].Assessment of consciousness
A patient’s level of consciousness provides information regarding function of the cerebral cortex and the ascending reticular activating system of the brainstem. Consciousness can be described as normal, depressed or obtunded, stuporous, or comatose. An animal in a stupor is partially or completely unconscious, but will respond to noxious stimuli. A patient in a coma is unconscious and cannot be roused with noxious stimuli. Coma typically indicates severe cerebral injury or brainstem damage, which carries a guarded prognosis.
Confirmation of injury and diagnosis
A diagnosis of traumatic brain injury is based primarily on a compatible history and clinical signs of intracranial neurologic dysfunction. However, additional tests can be used to confirm location and extent of injury. It is important to emphasize that advanced imaging of the brain — computed tomography (CT) and magnetic resonance imaging (MRI) — should be reserved for patients that do not respond to initial treatment or for patients who deteriorate despite aggressive therapy. Both imaging modalities require anesthesia, which can destabilize the head trauma patient, unless the patient is comatose on presentation.
Skull radiographs
Skull radiography may reveal calvarial fractures, but provides no information regarding the brain parenchyma. Radiographs can be difficult to interpret due to the irregularity of the skull bones and anesthesia is required for accurate positioning, which may be contraindicated in the acutely injured patient. However, radiography should not be limited to the skull following head trauma; images of the vertebral column, thorax, and abdomen are indicated to evaluate for evidence of other injuries.
Computed tomography
CT allows superior evaluation of bony structures and is preferred over conventional radiography, especially considering the 3D reconstruction capabilities [6]. Additionally, CT can be used to diagnose intracranial hemorrhage, alterations in ventricular size or shape, midline shift and edema. It does not provide good soft tissue detail of the brain parenchyma, but is frequently the preferred modality for evaluating humans with head trauma requiring surgical intervention because of the speed of image acquisition.
Magnetic resonance imaging
MRI allows superior soft tissue detail and is preferred for evaluation of the brain, especially the caudal fossa which does not image well with CT. MRI can detect subtle parenchymal changes which can be missed on CT and may provide information about prognosis. Hematomas or hemorrhage, parenchymal contusions, and edema are readily apparent on MRI images (Figure 3). A recent study correlated MRI findings with prognosis in veterinary head trauma patients and its use may therefore be of additional benefit [7]. Specifically, identification of mass effect and ventricular compression by parenchymal damage can be poor prognostic indicators and in such cases, decompressive surgery should be considered.

Treatment
Treatment of head trauma is proposed in a progressive tiered system based on the severity of injury and the success of the initial therapy (Figure 4). Tier 1 treatments are administered to all patients; Tier 2 treatments are administered to all patients with a MGCS of < 8 and failure of Tier 1 treatment; Tier 3 treatments are administered to all patients with a MGCS of < 8 and failure of Tier 2 treatments.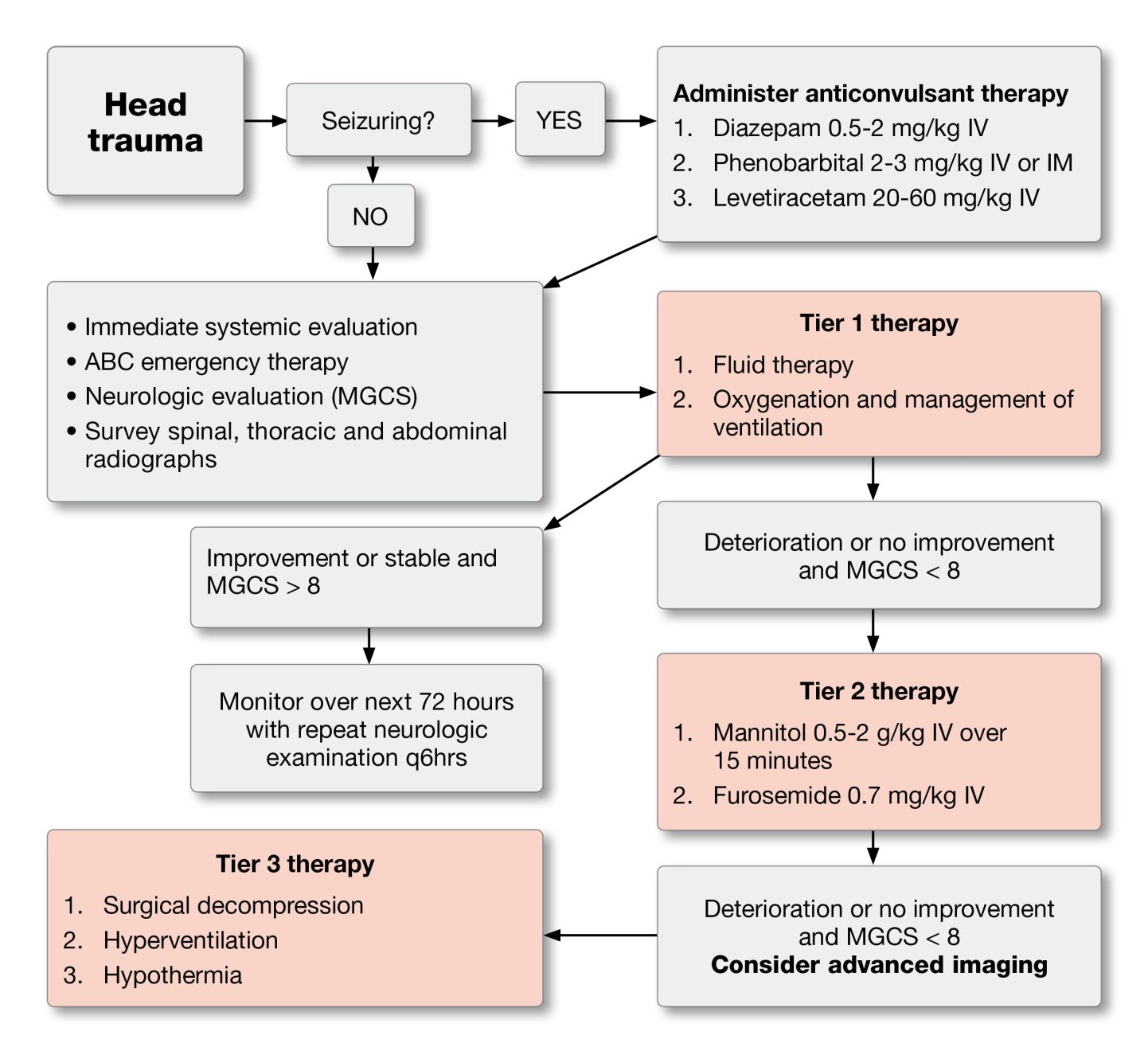
Tier 1 Therapy
Fluid Therapy
The goal of fluid therapy for the head trauma patient is to restore a normovolemic state; it is deleterious to dehydrate an animal in an attempt to reduce cerebral edema. Aggressive fluid therapy and systemic monitoring is required to ensure normovolemia and maintain adequate central perfusion pressure [1] [2] [3] [4] [8].
Crystalloid, hypertonic, and colloid fluids should be given concurrently to help restore and maintain blood volume following trauma. Crystalloids are usually given initially for the treatment of systemic shock. The shock dose of balanced electrolyte solutions is 60 mL/kg [1] [2] [3] [4] [8] and it is recommended that the calculated dose is given in fractions, initially administering 25-33% of the total volume with frequent reassessment of the patient for normalization of blood pressure, mentation and central venous pressure (if monitored), with additional fractions given as needed.
Hypertonic and colloid fluid therapy can rapidly restore blood volume using low volume fluid resuscitation; additionally, colloids remain in the vasculature longer than crystalloid fluids. These fluids should be used with caution, as without concurrent administration of crystalloid solutions dehydration can develop. Other benefits of hypertonic fluids include the ability to improve cardiac output, restore normovolemia, and reduce inflammation after trauma. Hypertonic saline may be preferred in hypovolemic, hypotensive patients with increased intracranial pressure (ICP) as it improves cerebral perfusion pressure and blood flow by rapidly restoring intravascular blood volume. Additionally, the high sodium content draws fluid from the interstitial and intracellular spaces, reducing intracranial pressure. Hypertonic saline is contraindicated with systemic dehydration and hypernatremia. Hypertonic saline only remains within the vasculature for about one hour; therefore, it should be followed by colloids to maximize its effects. A dose of 2-4 mL/kg of 7.5% NaCl should be given over 5-10 minutes in cats [1] [2] [3].
Colloids (i.e., Hetastarch, Dextran-70) allow for low volume fluid resuscitation especially if total protein concentrations are below 50 g/L or 5 g/dL. Colloids also draw fluid from the interstitial and intracellular spaces, but have the added benefit of staying within the intravascular space longer than crystalloids. Hetastarch is typically given at 2-4 mL/kg over 5-10 minutes, with frequent patient re-evaluation; a total dose of 20 mL/kg/day may be given. In addition to volume resuscitation, oxygen carrying capacity should be considered, especially if the PCV (packed cell volume) is < 30%.
Head trauma patients should be positioned to maximize arterial circulation to the brain and improve venous drainage; this is best achieved by elevating the animal’s head at an angle of 30°. It is important to ensure the jugular veins are not occluded and that no restrictive collars are placed around the neck, which will elevate intracranial pressure.
Oxygen therapy and management of ventilation
The goal of oxygen therapy and management of ventilation is to maintain PaO2 at least equal to 90 mmHg and the PaCO2 below 35-40 mmHg. If the patient is able to ventilate spontaneously and effectively, supplemental oxygen should be delivered via “flow-by”; confinement within an oxygen cage prevents frequent monitoring. Face masks and nasal catheters should be avoided if possible, as they can cause anxiety which may contribute to ICP elevation (Figure 5).
Cats with severe head injury require mechanical ventilation to maintain arterial blood gas concentrations at their optimal levels. The absolute indications for mechanical ventilation include loss of consciousness, rising PaCO2 above 50 mmHg and falling peripheral capillary oxygen saturation (SPO2) despite appropriate treatment [1] [2] [3] [4] [8].

Tier 2 therapy
Diuretics
Increased ICP can be aggressively addressed with the administration of osmotic diuretics such as mannitol, but they should not be given to any patient without being certain that the animal has been volume-resuscitated. If not, their use can precipitate acute renal failure, hence they are reserved as tier 2 therapies. After administration, mannitol expands the plasma volume and reduces blood viscosity, which improves cerebral blood flow and delivery of oxygen to the brain, and reduces ICP by decreasing edema. Vasoconstriction occurs as a sequel to the increased PaO2, which in turn helps to decrease ICP. Additionally, the osmotic effect of mannitol reduces extracellular fluid volume within the brain [1] [2] [3] [4] [8] and it assists in scavenging free radicals, which contribute to secondary injury processes [9].
Mannitol should be given as a bolus (0.5-2 g/kg) over 15 minutes to optimize the plasma expanding effect; continuous infusions increase the permeability of the blood brain barrier, exacerbating edema. Low doses of mannitol are as effective at decreasing ICP as higher doses, but may not last as long. Mannitol reduces brain edema about 15-30 minutes after administration and has an effect for approximately two to five hours. Repeated dosing can cause diuresis leading to reduced plasma volume, increased osmolarity, intracellular dehydration, hypotension, and ischemia, so adequate isotonic crystalloid and colloid therapy is critical to maintain hydration.
Administration of furosemide (0.7 mg/kg) prior to giving mannitol has a synergistic effect in lowering ICP. The use of mannitol should be reserved for critical patients (MGCS of < 8), a deteriorating patient, or a patient failing to respond to other treatment; there is currently no evidence to support the notion that mannitol is contraindicated if intracranial hemorrhage is present.
Seizure therapy
Tier 3 therapy
Hyperventilation
Hypothermia
Surgery
Supportive therapy
Simon Platt
BVM&S, MRCVS, Dip. ACVIM (Neurology), Dip. ECVN
Dr. Platt received his veterinary degree in 1992 from the University of Edinburgh, Scotland, following which he undertook an internship in Small Animal Medicine and Surgery at the Ontario Veterinary College, University of Guelph and a two-year period of private practice in England. Dr. Platt completed a residency in neurology and neurosurgery in 1998 at the University of Florida and is currently a Professor at the Department of Small Animal Medicine and Surgery at the University of Georgia.
References
- Dewey CW. Emergency management of the head trauma patient. Principles and practice. Vet Clin North Am Small Anim Pract 2000;30(1):207-225.
- Hopkins AL. Head trauma. Vet Clin North Am Small Anim Pract 1996;26(4):875-891.
- Adamantos S, Garosi L. Head trauma in the cat: 1. assessment and management of craniofacial injury. J Feline Med Surg 2011;13(11):806-814.
- Adamantos S, Garosi L. Head trauma in the cat: 2. assessment and management of traumatic brain injury. J Feline Med Surg 2011;13(11):815- 822.
- Platt SR, Radaelli ST, McDonnell JJ. The prognostic value of the Modified Glasgow Coma Scale in head trauma in dogs. J Vet Intern Med 2001;15(6):581-594.
- Platt SR, Radaelli ST, McDonnell JJ. Computed tomography after mild head trauma in dogs. Vet Rec 2002;151(8):243.
- Beltran E, Platt SR, McConnell JF, et al. Prognostic value of early magnetic resonance imaging in dogs after traumatic brain injury: 50 cases. J Vet Intern Med 2014;28(4):1256-1262.
- Syring RS. Assessment and treatment of central nervous system abnormalities in the emergency patient. Vet Clin North Am Small Anim Pract 2005;35(2):343-358.
- Yilmaz N, Dulger H, Kiymaz N, et al. Activity of mannitol and hypertonic saline therapy on the oxidant and antioxidant system during the acute term after traumatic brain injury in the rats. Brain Res 2007;1164:132-135.
Share on social media