Loading component...
Gastric dilatation and volvulus
Written by Emma Donnelly and Daniel Lewis
Gastric dilatation and volvulus (GDV) is a life-threatening condition which requires prompt diagnosis and treatment. Although cases have been reported in cats it is more commonly dogs that present with the condition, which involves gaseous distension of the stomach in association with rotation along the longitudinal axis.
Key Points
Gastric dilatation and volvulus is a life-threatening condition; prompt diagnosis and treatment are vital to reduce morbidity and mortality.
The pathophysiology of gastric dilatation is a complex subject and incompletely elucidated.
Gastric decompression is of the utmost importance when treating this condition, either by placement of a stomach tube or by percutaneous trocharization.
Serum lactate levels are a useful indicator of response to treatment; it is thought to be a positive indicator of survival if the level decreases by > 50% within the first twelve hours of therapy.
Introduction
Gastric dilatation and volvulus (GDV) is a life-threatening condition which requires prompt diagnosis and treatment. Although cases have been reported in cats it is more commonly dogs that present with the condition, which involves gaseous distension of the stomach in association with rotation along the longitudinal axis. Historically the mortality rate from the condition has been regarded as high; different studies put it between 15%-68% [1] [2] [3] [4] [5], but with improved understanding of the condition it is hoped that morbidity and mortality will be reduced in future.Predisposing factors
Predisposing factors for GDV include genetic and environmental factors. The condition is most commonly seen in large or giant breeds of dogs, but it can and does occur in smaller breeds. There is a recognized breed predisposition to GDV; at-risk animals include the Great Dane, German Shepherd, Standard Poodle and Irish Setter, although this is by no means an exhaustive list. One study suggested the condition was most prevalent in the Grand Bleu de Gascogne [6], although this is not a breed commonly encountered in practice. The risk of developing the condition increases with age, regardless of breed; one study (which focused on Irish Setters) found the risk was elevated by 33% with each year of age [7]. It has been suggested that stretching of the hepato-gastric ligament allows greater stomach mobility in older dogs [8] [9]. Any dog with an increased thoracic depth-to-width ratio is at greater risk of GDV; this may be due to the different anatomical relationship between the stomach and the esophagus in these animals, which may restrict their ability to remove air from the stomach [7]. An anxious temperament has also been perceived as a predisposing factor, and is commonly reported by owners of dogs who have developed GDV [8], whilst animals described by their owners as “happy” seem less likely to develop the condition [7]. Any dog that has a “first degree” relative (e.g., parents, offspring or siblings) with a history of GDV is also considered to be at higher risk [7]. All of the aforementioned points are likely to indicate genetic factors which predispose to the condition.
Risk of GDV has been linked to a number of environmental factors including dietary factors such as feeding one large meal a day, feeding from a height, and various ingredients within a diet, but cause-and-effect relationships have not been fully elucidated [10].
An increased risk of GDV following splenectomy has been described [11]. The study concerned does not suggest an association between the cause of splenectomy and GDV; rather it is postulated that removal of the spleen increases space within the abdomen, which may allow the stomach to have more mobility than previously and hence an increased risk of GDV [12]. Splenic torsion is a complication that can be encountered in patients presenting with GDV, likely to be caused by the spleen being pulled with the stomach as it rotates.
Pathophysiology of GDV
Dogs with GDV often present in shock and can experience more than one type of shock simultaneously, e.g., obstructive, distributive, cardiogenic and hypovolemic. The distended stomach can obstruct blood flow within the caudal vena cava, resulting in reduced blood volume returning to the heart. This results in a reduced preload and stroke volume, which subsequently affects cardiac output; this is often described as obstructive shock. Patients will frequently be tachycardic on admission, a compensatory response in an attempt to maintain cardiac output. Stress and pain should also be considered as factors in animals that present with tachycardia [15].
An increase in venous pressure within the abdomen results in sequestration of blood in the splanchnic and portal veins. This, together with the up-regulation of inducible nitrous oxide synthase (iNOS) and the release of vasoactive cytokines as a result of the gastric inflammation, leads to peripheral vasodilation which can cause further pooling of blood, worsening the condition [15]. These factors combine to cause mal-distributive shock.
Hypovolemic shock is not a major contributor in these patients, although as noted splenic torsion can occur with GDV, and if there is tearing of the short gastric arteries and veins hemoabdomen can result. A decrease in oral fluid intake can contribute to dehydration in these patients, but is unlikely to be substantial enough to affect blood pressure [15].
Cardiac compromise is closely connected with morbidity and mortality in dogs. Myocardial ischemia can develop as a consequence of global hypoperfusion; in addition some of the pro-inflammatory cytokines released as a result of the condition have a direct depressant effect upon the myocardium. ECG monitoring can give some indication of the presence of damage to the myocardium [16], as changes in electrical activity may be identified. Monitoring serum troponin levels can allow assessment of heart damage; increases in this biomarker indicate a worsening prognosis, but if the sample has to be sent to an external laboratory for analysis this limits its usefulness.
It has been suggested that cardiac arrhythmia and a degree of myocardial dysfunction is seen in 40% of GDV patients [1] [2] [15]. Life-threatening arrhythmias do not necessarily present prior to surgical correction of the condition; they can arise up to 72 hours later. One study suggested that dogs diagnosed with a cardiac arrhythmia prior to surgery had a 25-38% increase in mortality rate [2]. The presence of an arrhythmia is not necessarily a deciding factor on whether the patient should have surgical intervention or euthanasia, but it is a factor to be considered alongside a full clinical examination and history to enable a more accurate prognosis for the patient.
Patients may show signs of respiratory distress, such as increased respiratory rate and effort. This may be as a result of increased stomach size. Normally, the diaphragm moves caudally during inspiration, but this is prevented if the stomach is enlarged [17] and the decrease in intrathoracic volume can reduce tidal volume and lead to a ventilation/perfusion mismatch. Aspiration pneumonia is also a risk; this can be present prior to surgery or develop as a post-operative complication, and can be associated with a less favorable outcome. If pulmonary function is severely affected by either of these problems then hypoxemia can result, to the further detriment of the patient.
Diagnosis
Diagnosis is generally based on signalment, history and clinical examination. Owners commonly report unproductive retching and hypersalivation, although abdominal distension and collapse can be the first signs noticed by an owner. On clinical examination there may be evidence of hypoperfusion: tachycardia, weak peripheral pulses, and pale mucous membranes with a capillary refill time (CRT) greater than two seconds. However, as the patient may be displaying signs indicative of distributive shock, the mucous membranes may be injected with a rapid CRT. Abdominal distension may be obvious on visual assessment and tympany may be noted on abdominal percussion. However, in deep-chested dogs it can be difficult at times to discern if the stomach is tympanitic, as it may lie within the costal arch (Figure 2).

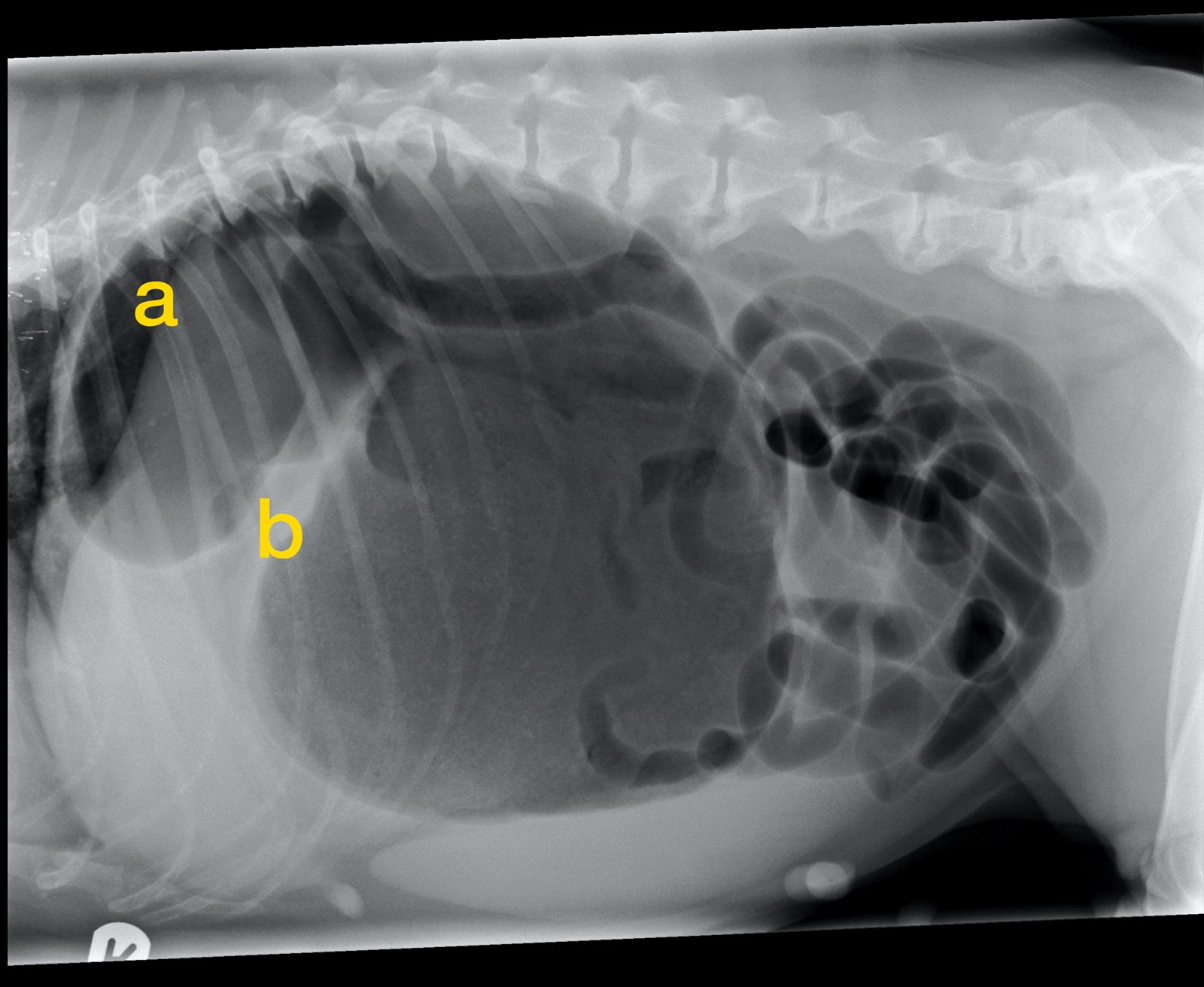
Diagnostic imaging will confirm if torsion is present or if the patient has gastric dilatation alone; this is important as dilatation may not require immediate surgery. A single right lateral abdominal radiograph is usually diagnostic; with classic GDV there will be two gas-filled structures visible in the cranial abdomen (Figure 3). The larger one is the gastric fundus, with the pylorus appearing as a smaller gas-filled structure dorsally. The two gas-filled areas may be separated by a band of soft tissue. Thoracic radiographs are also useful as they may give an early indication of aspiration pneumonia and allow prompt use of antimicrobials [18].
Initial therapy
IIt is important to record the initial clinical findings to assess response to treatment: heart rate, respiratory rate, pulse quality, mucous membrane color, capillary refill time and, if possible, blood pressure. A large-bore intravenous catheter should be placed (normally into the cephalic vein) as soon as possible and fluid therapy commenced. In large dogs it can be difficult to give an adequate fluid volume rapidly enough to increase preload with one catheter, therefore placing two catheters, one in each cephalic vein, can be beneficial. The rate of the fluid therapy will depend on the clinical findings and any other underlying health conditions, but in general crystalloids at 90 mL/kg/hour (shock rate) is recommended, with vital parameters assessed every 15 minutes. However it can be more appropriate to administer smaller volumes as a bolus (e.g., 20 mL/kg of fluid given over 15 minutes) with frequent reassessment, adjusting the dose as necessary. A full opioid agonist (e.g., methadone at 0.2-0.3 mg/kg IV) should be given as early as possible [19].
Rapid gastric decompression is of the utmost importance because the risks of hypoxemia are so great. Placement of a stomach tube or decompression by percutaneous trocharization are both suitable options. One study comparing the two techniques concluded that neither had a high complication rate and both were found generally to be successful [20]. Surgical intervention should proceed once the patient is stable, which will be determined by clinical examination, such as a resolution of tachycardia and normalization of cardiovascular parameters.
Laboratory findings
Surgical procedure
Premedication and anesthetic induction agent are at the discretion of the clinician. Generally methadone should be adequate for initial pain relief. Anesthesia should be maintained with either isoflurane or sevoflurane; nitrous oxide should not be given to a GDV patient, as it will accumulate in gas-filled spaces and can therefore worsen the gastric dilatation. Since the dog may regurgitate when the stomach position is corrected, it can be useful to have suction equipment ready for use. Given that gastro-esophageal reflux is a known risk factor for esophagitis and esophageal stricture formation post-operatively, the use of omeprazole (1 mg/kg IV) prior to induction may reduce the risk of this occurring [17].
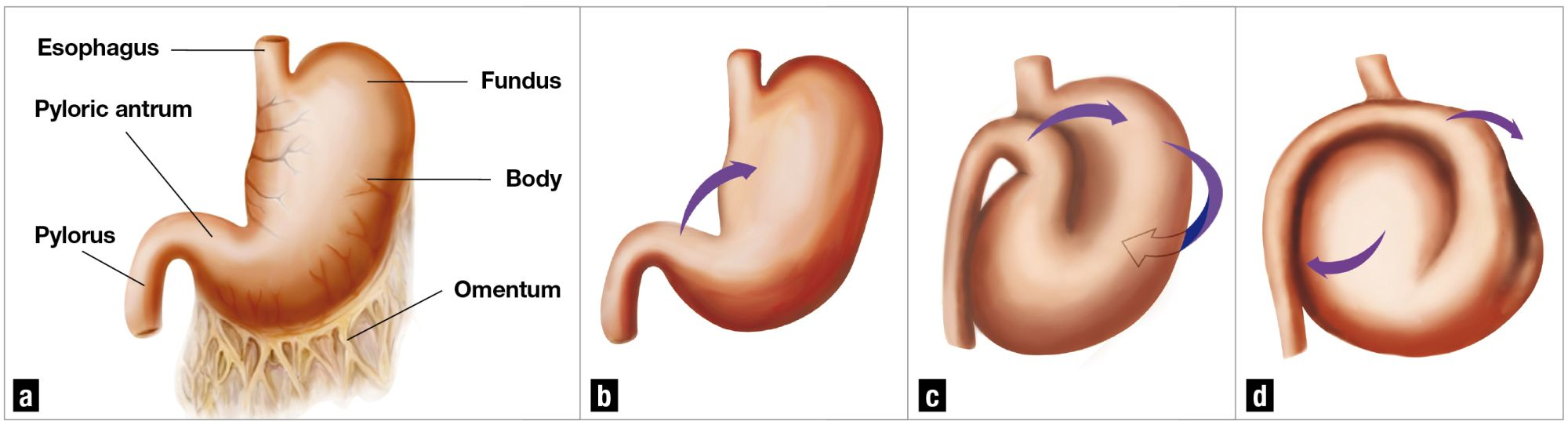
The aim of surgery is to de-rotate the stomach. The torsion is typically clockwise (when viewed from behind the animal) and on incision the omentum will usually be covering the stomach. Gaseous distension noted at this point can be easily drained using a needle or cannula attached to the surgical suction tubing. The surgeon should locate the pylorus (often found dorsally on the left-hand side of the abdomen), and grasp it with one hand whilst the other hand holds the fundus of the stomach. The fundus should then be pushed towards the operating table whilst the pylorus is manipulated up towards the incision and over to the right side of the abdomen. This simultaneous pushing and pulling should correct the stomach position (Figure 4).

After correcting the stomach position it should be fixed to the body wall to prevent recurrence. Various gastropexy techniques have been described; the most frequently used is known as “incisional gastropexy”. With this technique an incision is made in the seromuscular layer of the gastric wall, parallel to the long axis of the stomach, at the level of the pyloric antrum. Another incision of the same length is made in the right transversus abdominus muscle and the incisions are sutured together using an absorbable monofilament suture, with the aim of forming an adhesion which prevents repeat torsion in future [22].
Complications that affect prognosis
At surgery the stomach should be assessed for color, wall thickness and blood supply, and the viability of the tissue assessed; any areas of necrosis or impaired viability should be resected. The spleen should also be examined; if the splenic artery or vein are damaged, or there is active bleeding, a splenectomy should be performed. Post-operative mortality is significantly increased in patients that require gastric resection or splenectomy; one study found that partial gastrectomy was not associated with an increased risk of death, but the risk of post-operative complications was increased [3]. In patients where there is marked gastric necrosis, such that resection is not possible, euthanasia will be required. It should be emphasized that euthanasia may be the preferred option for some patients, either because of the financial outlay involved or because there is severe concurrent disease. The clinician should discuss fully the risks, costs and potential outcomes with the owner before embarking on surgery.
Post-operative care
Patients which are severely hypoperfused prior to anesthesia may be slow to recover from surgery and can require intensive supportive care. Once perfusion is restored patients can develop post-operative complications related to IRI. This is associated with increased mortality, as myocardial damage can result in the development of arrhythmias. ECG monitoring should be continued in the post-operative period as cardiac arrhythmias are common following GDV; the most frequent are ventricular in source, although supra-ventricular arrhythmias can also occur. If these are considered significant, the treatment of choice is lidocaine administered as a bolus of 2 mg/kg (repeated up to a total of 8 mg/kg) followed by a continuous rate infusion (at 25-75 µg/kg/min). At least one study has evaluated the pre-emptive use of lidocaine treatment for dogs with GDV [23]; given as a bolus prior to decompression and initiation of fluid therapy, lidocaine reduced damage from IRI, lessened the risks of complications developing, and resulted in a decreased mortality rate.
In patients requiring extensive gastric resection placement of an esophageal feeding tube may be of benefit. Nausea post-operatively can be treated with medication such as maropitant. Pain relief will be dependent on the individual patient; opioids such as methadone can be given in the initial post-operative phase, with transition to buprenorphine when possible. NSAIDs should be avoided due to the risks of gastric wall compromise and renal dysfunction. Fluid therapy should be continued until the patient is eating and drinking.
Conclusion
Emma Donnelly
BSc, BVMS, Dip. ECVECC, MRCVS, Vets Now 24/7 Emergency & Specialty Hospital, Glasgow, UK
United Kingdom
Dr. Donnelly graduated from Glasgow University in 2013 before undertaking a rotating internship at the city’s Vets Now Clinic, a center dedicated to out of hours and specialist provision. During this time, she developed an interest in ECC, and she went on to complete a discipline-specific internship followed by a residency in ECC. She returned to Vets Now in 2020, where she currently works as an ECC consultant and residency supervisor, with her main areas of interest being neonatal and pediatric medicine.
Daniel Lewis
MA, VetMB, CertVA, Dip. ACVECC, MRCVS
United Kingdom
Following graduation from Cambridge Vet School in 1995, Dr. Lewis worked in mixed practice for five years, where he gained his Certificate in Veterinary Anaesthesia. He then spent eight years at a large hospital-based emergency clinic in Manchester, before undertaking a residency at the Royal Veterinary College in London, obtaining his Diploma in Emergency and Critical Care in 2011. Dr. Lewis joined Vets-Now Referrals in 2015 and has a particular interest in feline medicine and septic patients.
References
- Brockman DJ, Washabau RJ, Drobatz KJ. Canine gastric dilatation-volvulus syndrome in a veterinary critical care unit: 295 cases (1986-1992). J Am Vet Med Assoc 1995;207:460-464.
- Bourman JD, Schertel ER, Allen DA, et al. Factors associated with perioperative mortality in dogs with surgically managed gastric dilatationvolvulus: 137 cases (1988-1993). J Am Vet Med Assoc 1996;208:1855- 1858.
- Beck JJ, Staatz AJ, Pelsue DH, et al. Risk factors associated with short-term outcome and development of perioperative complications in dogs undergoing surgery because of gastric dilatation-volvulus; 166 cases (1992-2003). J Am Vet Med Assoc 2006;299:1934-1939.
- Muir WW. Gastric dilatation-volvulus in the dog, with emphasis on cardiac arrhythmias. J Am Vet Med Assoc 1982;180:739-742.
- Glickman LT, Lantz GC, Schellenberg DB, et al. A prospective study of survival and recurrence following the acute gastric dilatation volvulus syndrome in 136 dogs. J Am Anim Hosp Assoc 1998;34(3):253-259.
- Evans KM, Adams VJ. Mortality and morbidity due to gastric dilatation-volvulus syndrome in pedigree dogs in the UK. J Small Anim Pract 2010;51;376-381.
- Schellenberg DB, Yi Q, Glickman NW, et al. Influence of thoracic conformation and genetics on the risks of gastric dilatation and volvulus in Irish Setters. J Am Anim Hosp Assoc 1998;34:64-73
- Bell JS. Inherited and predisposing factors in the development of gastric dilatation and volvulus in dogs. Topics Comp Anim Med 2014;29(3):60-63.
- Hall JA, Willer RI, Seim HB, et al. Gross and histological evaluation of hepatogastric ligaments in clinically normal dogs and dogs with gastric dilatation-volvulus. Am J Vet Res 1995;56:1611-1614.
- Raghavan M, Glickman NW, Glickman LT. The effect of ingredients in dry dog foods on the risk of gastric dilatation-volvulus in dogs. J Am Anim Hosp Assoc 2006;42:28-36.
- Sartor AJ, Bentley AM, Brown DC. Association between previous splenectomy and gastric dilatation-volvulus in dogs: 453 cases (2004-2009). J Am Vet Med Assoc 2013;242:1381-1384.
- Millis DL, Nemzek J, Riggs C. Gastric dilatation-volvulus after splenic torsion in two dogs. J Am Vet Med Assoc 1995;207:314-315.
- Van Kruiningen HJ, Gargamelli C, Havier J, et al. Stomach gas analyses in canine acute gastric dilatation and volvulus. J Vet Intern Med 2013;27;1260- 1261.
- Glickman LT, Glickman NW, Schellenberg DB, et al. Non-dietary risk factors for gastric dilatation-volvulus in large and giant breeds of dogs. J Am Vet Med Assoc 2000;217(10):1492-1499.
- Sharp CR, Rozanski EA. Cardiovascular and systemic effects of gastric dilatation and volvulus in dogs. Topics Comp Anim Med 2014;29(3):67-70.
- Adamik KN, Burgener IA, Kovacevic A, et al. Myoglobin as a prognostic indicator for outcome in dogs with gastric dilatation and volvulus. J Vet Emerg Crit Care 2009;19(3):247-253.
- Sharp CR. Gastric dilatation-volvulus. In: Silverstein DC, Hopper K (eds). Small Animal Critical Care Medicine. Missouri, Elsevier Inc. 2009;584-588.
- Green JL, Cimino Brown D, Agnello KA. Preoperative thoracic radiographic findings in dogs presenting for gastric dilatation-volvulus (2000-2010): 101 cases. J Vet Emerg Crit Care 2012;22:595-600.
- Ramsay I. BSAVA Small Animal Formulary 8th Ed. Gloucester: BSAVA 2014;248-249.
- Goodrich ZJ, Pavell L, Hulting KJ. Gastric decompression. J Small Anim Pract 2013;54:75-79.
- Green TI, Tonozzi CC, Kirby R, et al. Evaluation of plasma lactate values as a predictor of gastric necrosis and initial and subsequent plasma lactate values as a predictor of survival: 84 dogs (2003-2007). J Vet Emerg Crit Care 2011;21(1):36-44.
- Radlinsky MAG. Gastric Dilatation-volvulus. In: Fossum TW (ed). Small Animal Surgery (4th ed) Missouri: Mosby, Inc. 2013;482-487.
- Bruchim Y, Itay S, Shira BH, et al. Evaluation of lidocaine treatment on frequency of cardiac arrhythmias, acute kidney injury and hospitalization time in dogs with gastric dilatation volvulus. J Vet Emerg Crit Care 2012;22:419- 427.
- Monnet E. Gastric dilatation-volvulus syndrome in dogs. Vet Clin North Am Small Anim Pract 2003;33(5):987-1005.
Other articles in this issue
Share on social media